USMLE-STEP-3 Online Practice Questions and Answers
A22-year-old male presents to an acute care clinic in order to have two genital lesions evaluated. He first noticed the lesions about 2 weeks ago, but delayed seeking medical care because he believed they were harmless due to the lack of any discomfort. He states that he does engage in unprotected sexual intercourse, with the most recent time being 1 month ago. On examination, the glans penis features two distinct nontender papules with elevated edges surrounding ulcerated craters. They each measure 1 cm in diameter. There is also nontender bilateral inguinal lymphadenopathy.
Which of the following is true about this patient's condition?
A. The causative agent is a virus.
B. Light microscopy of fluid from the lesions will reveal gram-negative rods in chains.
C. The presence of multiple distinct lesions is uncommon.
D. There is a latent phase in which patients are asymptomatic.
E. Although associated with persistent symptoms if left untreated, it does not carry a significant risk for mortality.
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101°F. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
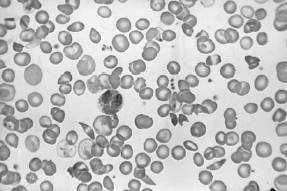
.
Among the initial orders for this patient should be which of the following?
A. broad-spectrum antibiotics for community-acquired pneumonia
B. type and hold for 2 units packed RBCs
C. an arterial blood gas
D. a CT scan of the abdomen
E. analgesics
Which of the following is the most appropriate treatment for a 32-year-old male with a toxic nodular goiter and compressive airway symptoms?
A. radioactive iodine therapy
B. propranolol
C. propylthiouracil
D. Lugol's solution
E. total lobectomy
Afather and son come to your office because of persistent diarrhea. They relate the presence of watery diarrhea for over 2 weeks. They noted that the diarrhea began after returning from a Boy Scout camping trip in the Rocky Mountains. The diarrhea has waxed and waned for 2 weeks. It is nonbloody and foul smelling. They have had increased flatulence and mild abdominal cramping.
What would be the most appropriate treatment?
A. oral ciprofloxacin
B. oral metronidazole
C. bismuth subsalicylate (Pepto-Bismol)
D. an antidiarrheal agent only; no antimicrobials necessary
E. oral rehydration only
You are working in a community clinic on a Native American reservation. A mother brings in her 8-year-old son for an ophthalmic evaluation. On examination, you find bilateral corneal ulceration and decreased visual acuity. What is the most common infectious cause of blindness in the world?
A. HSV
B. C. trachomatis
C. GAS
D. S. pneumoniae
E. E. coli
A mother brings her 4-year-old son to your office, relating that he fell earlier that morning while at the playground. She says that the boy tripped over another child and landed on his outstretched hands. On examination, the boy has some mild swelling around his left wrist, and he says that it hurts when you palpate it. What is the most appropriate next step?
A. Call the department of Children's Protective Services to investigate the accident.
B. Attempt a nursemaid's elbow reduction.
C. Perform anterior-posterior (AP) and lateral x-rays of the left wrist and elbow.
D. Wrap the wrist in an Ace wrap, and put the arm in a sling.
E. Order a magnetic resonance imaging (MRI) of the wrist looking for a growth plate injury.
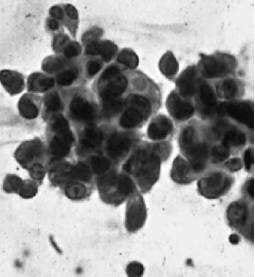
A 42-year-old woman who previously underwent a vaginal hysterectomy for persistent cervical dysplasia presents to your office for vaginal cytology. Her vaginal cytology is shown in Figure.
Which of the following is the most appropriate next step in management?
A. repeat vaginal cytology in 6 months
B. observation
C. random vaginal biopsies
D. intravaginal estrogen cream followed by repeat cytology
E. colposcopic examination of the vaginal canal
A 25-year-old nulligravid woman presents as a new patient to your gynecology practice. She has recently moved to the area. She is a healthy woman with no medical problems and is currently using oral contraceptives without problems. She informs you that she and her husband are planning to start a family within the next year. On review, you find her family history is unremarkable, but she informs you that her husband's sister has cystic fibrosis.
What is the approximate prevalence of cystic fibrosis carrier state in White individuals?
A. 1in10
B. 1in25
C. 1in50
D. 1in100
E. 1in200
A38-year-old married woman presents to her urgent care clinic complaining of "crying spells" for several weeks since the termination of her employment. She admits to feeling "down all the time." She also has difficulty falling asleep, poor energy, decreased appetite, and is "not able to enjoy anything." She fears that her condition will never improve. She has begun to feel that "it wouldn't matter if I died," but she denies any suicidal plan or intent. She drinks one to two mixed drinks per week and denies any drug use. It is decided to begin antidepressant therapy with paroxetine (Paxil) 20 mg at bedtime.
Which of the following side effects would be most likely to emerge after several months of treatment?
A. headache
B. inhibited orgasm
C. loose stools
D. nausea
E. vivid dreams
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
Total cholesterol: 235 mg/dL Triglycerides: 210 mg/dL HDL cholesterol: 45mg/dL LDL cholesterol: 162 mg/dL
He states that he has not had any immunizations in "longer than I can remember." Which of the following would be recommended for him?
A. hepatitis A and hepatitis B vaccines
B. herpes zoster vaccine (Zostavax)
C. tetanus, diphtheria, and acellular pertussis (Tdap) vaccine
D. tetanus and diphtheria (Td) vaccine
E. Tdap and PPV-23