USMLE-STEP-1 Online Practice Questions and Answers
Referring to following figure, arrow 2 indicates which of the following structures?
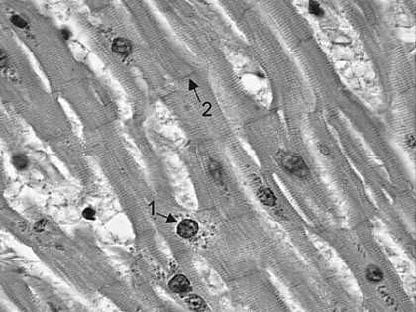
A. intercalated disk
B. motor end-plate
C. sarcoplasmic reticulum
D. tendinous junction
E. transverse tubule or T tubule
Patients with functional dyspepsia (disturbed indigestion) and prominent nausea frequently experience spurts of excessive acid exposure to the upper duodenum. This results in pancreatic secretion, mainly through the action of which of the following substances?
A. cholecystokinin
B. gastrin
C. glucagon
D. secretin
E. vasoactive intestinal polypeptide (VIP)
Lipoxygenase converts arachidonic acid to biologically active compounds called leukotrienes. Leukotrienes have been implicated in several disease entities, including allergic asthma, where they are presumed to mediate bronchoconstriction. Introducing leukotrienes into an airway would be expected to cause which of the following responses?
A. decreased airway resistance
B. decreased dead space volume
C. increased functional residual capacity (FRC)
D. increased lung compliance E. increased total lung capacity
A patient with newly diagnosed schizophrenia is given chlorpromazine. It is a drug that has amongst other effects moderate anticholinergic activity. As a consequence, which of the following is an expected side effect of this medication?
A. bradycardia
B. decreased GI sphincter tone
C. dry mouth
D. emptying of urinary bladder
E. increased GI motility
The rate-limiting step in glycolysis occurs at the step catalyzed by which of the following enzymes?
A. glyceraldehyde-3-phosphate dehydrogenase
B. 6-phosphofructo-1 kinase, PFK-1
C. 6-PFK-2
D. phosphoglycerate kinase
E. pyruvate kinase
Which of the following is true with respect to the actions of the mineralocorticoids?
A. decrease carbohydrate metabolism
B. increase appearance of the secondary sex characteristics
C. increase synthesis of androgens
D. regulate aldosterone secretion
E. regulate sodium retention by the kidneys
The parents of a 1-year-old boy are alarmed at the increasing frequency of their child biting his lips and finger tips. In addition, on several occasions they have noticed what appear to be particles of "orange sand" in their son's diapers. They report to their pediatrician that they believe their child is delayed in acquiring motor skills such as holding up his head and sitting unaided. Clinical tests performed on serum and urine indicate a threefold increase in serum uric acid and a tenfold elevation in the urinary ratio of uric acid to creatinine. These findings are suggestive of which of the following disorders?
A. adenosine deaminase deficiency
B. adenylosuccinate lyase deficiency
C. Lesch-Nyhan disease
D. purine nucleotide phosphorylase deficiency
E. orotic aciduria
The ability of the liver to regulate the level of blood glucose is critical for survival. Anumber of sources of carbon atoms of nonhepatic origin are used by the liver for gluconeogenesis. However, the net conversion of carbons from fat into carbons of glucose cannot occur in humans because of which of the following?
A. Fat oxidation occurs in the mitochondria and gluconeogenesis occurs in the cytosol.
B. States of catabolism and anabolism are never concurrently active.
C. Storage of fats occurs in adipose tissue and gluconeogenesis occurs in liver and kidney.
D. The carbons of acetyl-CoA from fat oxidation are lost as C in the TCA cycle.
E. The carbons of acetyl-CoA from fat oxidation inhibit conversion of pyruvate to oxaloacetate.
A 32-year-old man is admitted for neuropsychiatric evaluation after exhibiting bizarre behavior. During his medical workup, he is found to have cirrhosis and a mild parkinsonian tremor. Which of the following diagnoses provides the best explanation for these findings?
A. congenial hepatic fibrosis
B. peliosis hepatis
C. primary sclerosing cholangitis
D. Reye syndrome
E. Wilson disease
A 17-year-old patient suffers from tonicclonic seizures. This condition has been well controlled with a regimen of phenytoin. Which of the following signs or symptoms indicates phenytoin toxicity?
A. diplopia and abnormal gait
B. hyperprolactinemia
C. polydipsia and polyuria
D. postural hypotension
E. rigidity and tremor